Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a group of progressive lung disorders that cause airflow limitation and breathing difficulties. More than 16 million Americans have been diagnosed with COPD, while many others remain undiagnosed. The most common forms of COPD are emphysema and chronic bronchitis. Although COPD cannot be cured, symptoms can often be managed with medications and supportive treatments. Smoking tobacco is the leading cause of COPD because it creates permanent damage to lung tissue and may also contribute to lung cancer development.
Other causes and risk factors for COPD include:
- Long-term exposure to dust, smoke, fumes, and chemical irritants
- Air pollution and occupational hazards such as mining exposure
- Asthma, which may increase the risk of developing COPD later in life
- Genetic conditions such as alpha-1 antitrypsin deficiency
COPD can lead to serious and potentially life-threatening complications, including:
- Chronic cough with mucus production
- Shortness of breath
- Bronchoconstriction
- Hypoxia or hypoxemia
- Pneumonia
- Respiratory distress, failure, or arrest
- Altered mental status
- Severe dyspnea with minimal activity
COPD causes airway obstruction through inflammation, mucus buildup, and narrowing of the air passages. Damage to the alveoli further interferes with oxygen exchange. As the disease progresses, many patients experience worsening symptoms and may eventually require long-term supplemental oxygen therapy.
EMS and COPD
Respiratory emergencies are among the most common reasons EMS is activated. Studies estimate that approximately 12% of EMS calls involve respiratory distress. EMS providers play a critical role in recognizing COPD exacerbations and initiating early treatment. Prompt interventions can improve symptoms, prevent deterioration into respiratory failure, and reduce the need for invasive airway management.
Because respiratory distress may result from many different conditions, accurate assessment is essential for selecting appropriate treatment.
Anatomy and Physiology of COPD
Upper Respiratory Tract
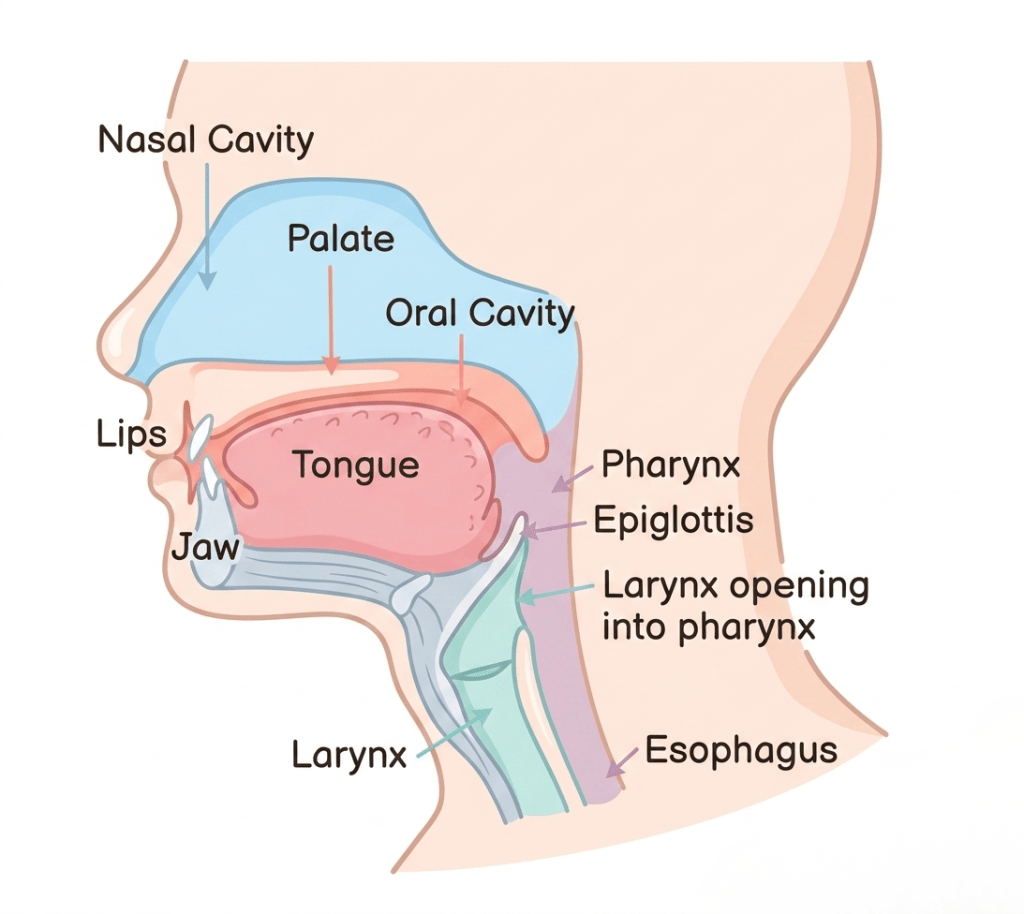
The respiratory system is divided into upper and lower airways, separated by the larynx.
Structures of the Upper Airway
- Pharynx: Passageway connecting the mouth and nasal cavity to the esophagus and trachea
- Oropharynx: Includes the mouth and throat
- Nasopharynx: Area behind the nasal cavity
- Laryngopharynx: Region where food and air separate into the esophagus and trachea
- Larynx: Contains the vocal cords and protects the lower airway
- Epiglottis: Cartilage flap that closes during swallowing to prevent aspiration
- Vocal cords: Can close reflexively to protect the airway
- Esophagus: Muscular tube carrying food and liquids to the stomach
Lower Respiratory Tract
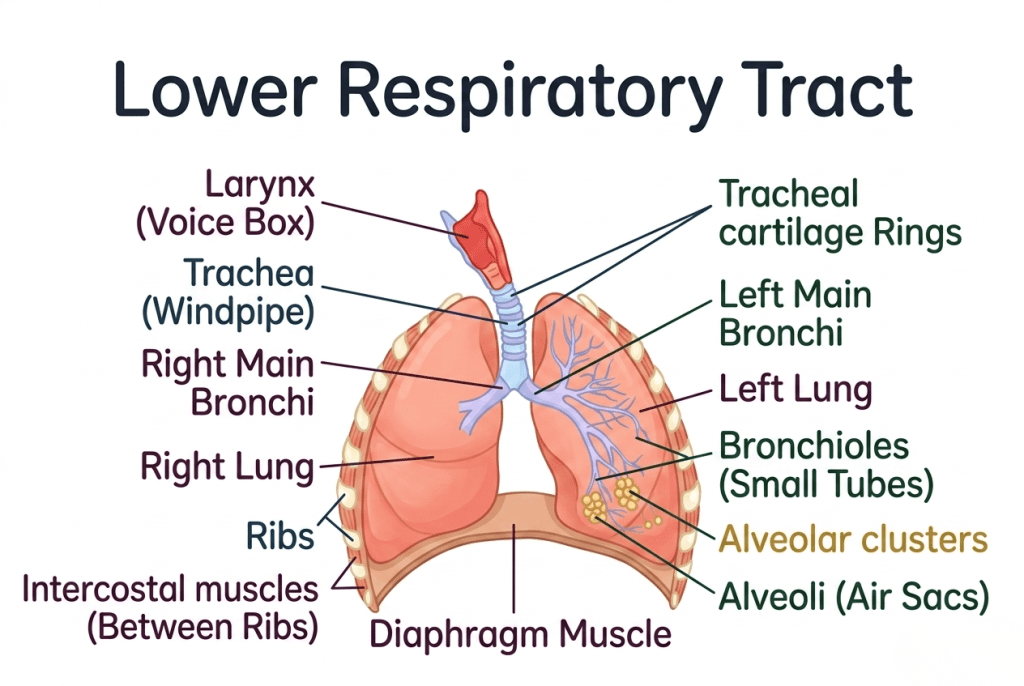
The lower airway allows air to travel into the lungs where gas exchange occurs.
Structures of the Lower Airway
Trachea:
The main airway extending from the larynx to the carina.
Carina:
Point where the trachea divides into the right and left bronchi.
Bronchi:
Large conducting airways branching into the lungs.
Bronchioles:
Small muscular airways capable of constricting or dilating.
Alveolar ducts:
Small passages leading to the alveoli.
Alveoli:
Tiny air sacs where oxygen and carbon dioxide exchange occurs across thin membranes.
Supporting Respiratory Structures
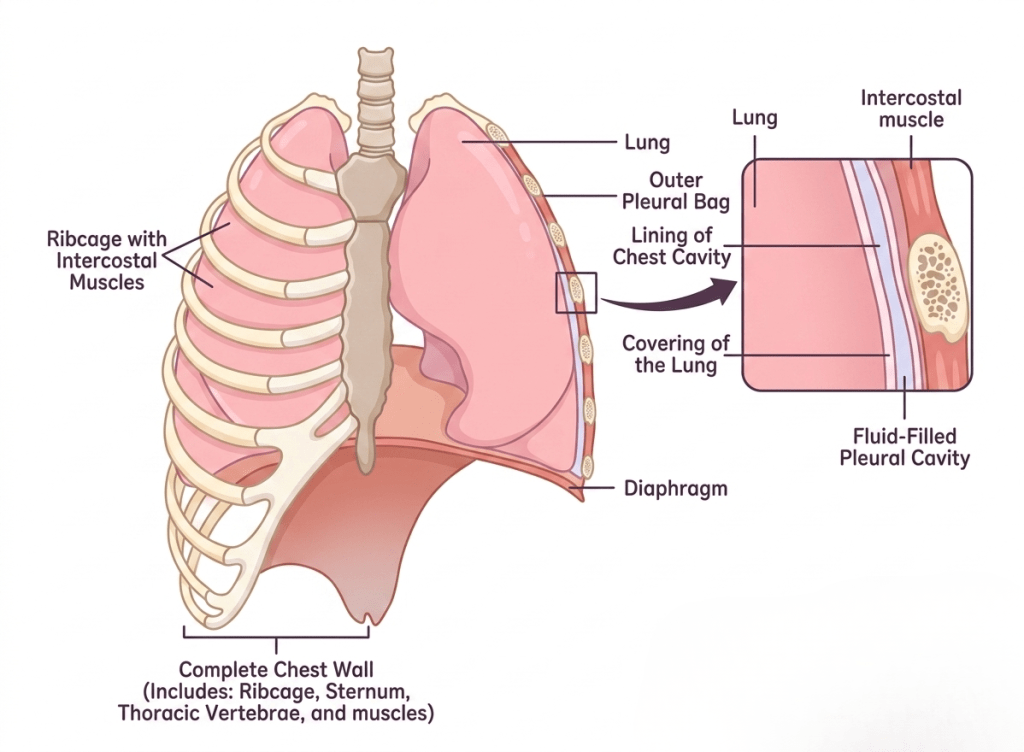
Diaphragm
Primary muscle responsible for breathing. During inhalation it contracts, lowering thoracic pressure and pulling air into the lungs. During exhalation it relaxes, allowing air to leave the lungs.
Ribs and Intercostal Muscles
Provide protection and assist chest expansion during breathing.
Pleural Space
Potential space between the lungs and chest wall containing lubricating fluid. Air or fluid accumulation in this space may impair lung function.
Respiratory Physiology
The respiratory system supplies oxygen to body tissues and removes carbon dioxide produced during metabolism. Gas exchange occurs through diffusion, where molecules move from areas of higher concentration to lower concentration.
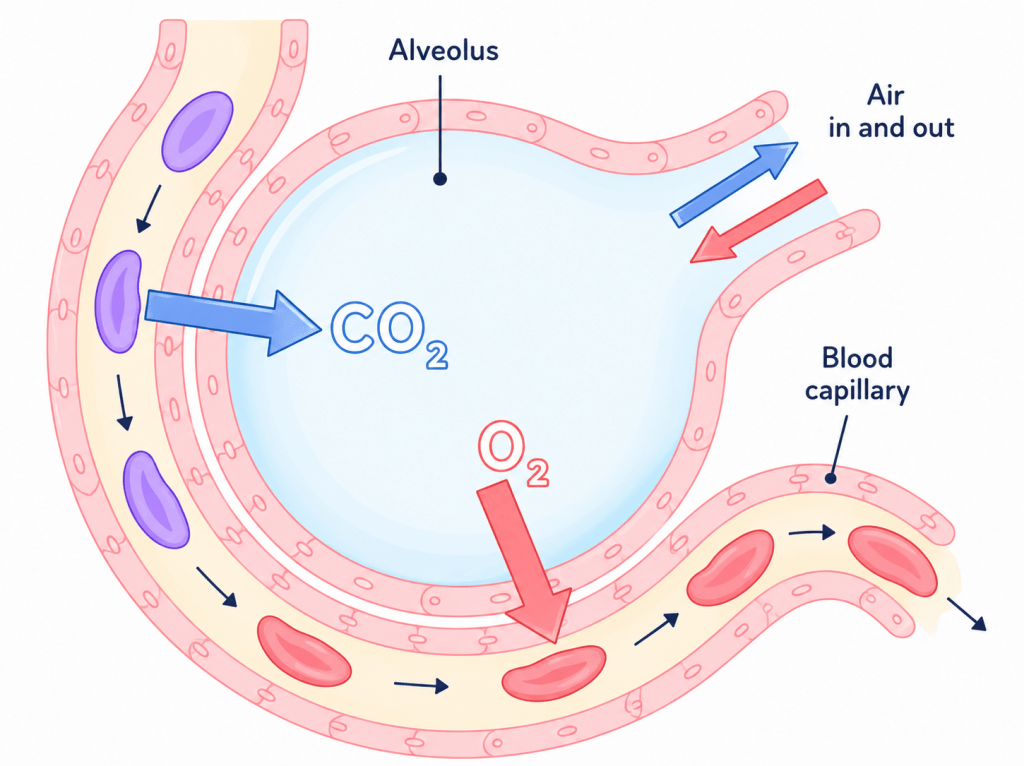
In the lungs:
- Oxygen moves from the alveoli into pulmonary capillaries
- Carbon dioxide moves from the blood into the alveoli to be exhaled
The alveolar-capillary membrane is extremely thin, allowing efficient gas exchange.
Common Respiratory Terms
- Tidal volume: Amount of air moved during normal breathing
- Residual volume: Air remaining after maximum exhalation
- Inspiratory reserve volume: Extra air inhaled after a normal breath
- Expiratory reserve volume: Additional air exhaled after normal exhalation
- Vital capacity: Maximum amount of air exhaled after full inhalation
- Dead space: Air that does not participate in gas exchange
- Surfactant: Substance that prevents alveolar collapse
Acid-Base Balance
The respiratory system helps regulate body pH by controlling carbon dioxide levels. Carbon dioxide forms carbonic acid in the bloodstream, making it an important acid-base regulator.
Increased breathing removes more carbon dioxide, while decreased breathing allows carbon dioxide to accumulate.
COPD and Its Effects on the Lungs
COPD progressively damages lung tissue over time.
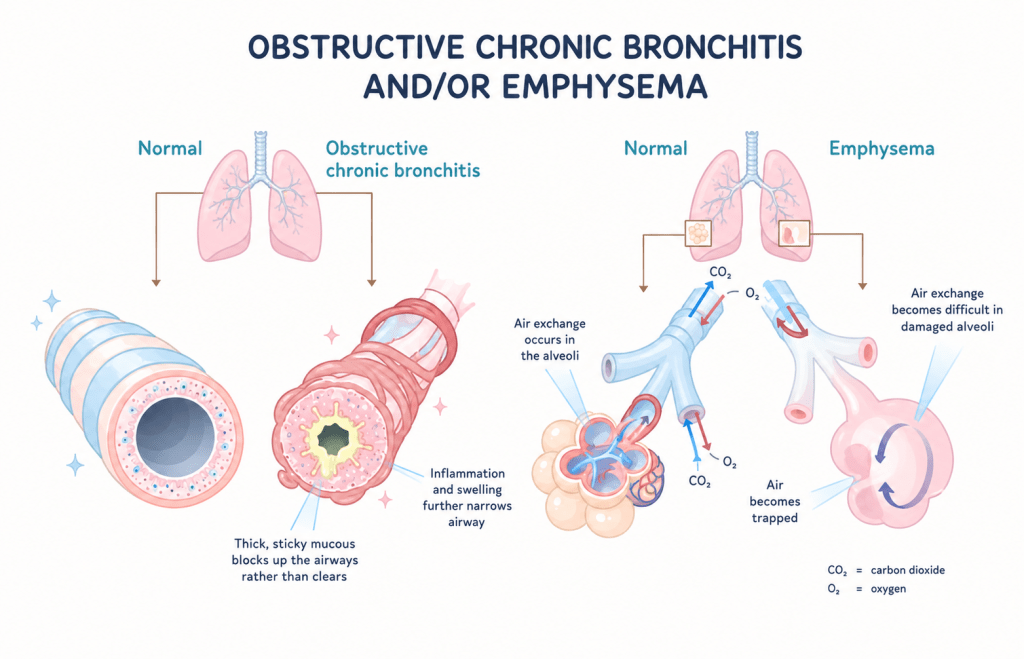
Chronic Bronchitis
Chronic bronchitis mainly affects the bronchi and bronchioles. Persistent inflammation leads to mucus production, airway narrowing, and chronic cough. Airflow obstruction commonly causes wheezing and breathing difficulty.
Emphysema
Emphysema damages the alveoli, causing them to lose elasticity and shape. Air becomes trapped in the lungs because exhalation is impaired. Chronic air trapping may eventually create a “barrel chest” appearance. Fewer healthy alveoli remain available for gas exchange, increasing the risk of hypoxia and respiratory distress.
Recognition
Patients with COPD often function normally day to day but may experience exacerbations that worsen breathing symptoms.
Common Triggers
- Physical exertion
- Smoke or air pollutant exposure
- Continued smoking
- Respiratory infections
Signs and Symptoms
Symptoms may include:
- Dyspnea
- Rapid breathing
- Tachycardia
- Anxiety
- Nausea or vomiting
- Productive or dry cough
- Wheezing or diminished lung sounds
- Hypoxia or cyanosis
- Altered mental status
- Chest tightness or discomfort
- Accessory muscle use or retractions
Typical COPD exacerbations often present with wheezing, shortness of breath, and hypoxia.
Assessment
A thorough assessment is important to identify the cause of respiratory distress.
Helpful Questions
- Has this happened before?
- Have home treatments helped?
- Is oxygen used regularly at home?
- Any recent illness or infection?
- Are symptoms becoming more frequent?
Physical Assessment Findings
Assess for:
- Wheezing or diminished lung sounds
- Chest wall tenderness or instability
- Accessory muscle use
- External trauma
- Cyanosis or poor perfusion
Consider other causes of respiratory distress such as:
- Pneumonia
- CHF or pulmonary edema
- Pulmonary embolism
- Asthma
- Anxiety
- Anaphylaxis
- Myocardial infarction
Treatment and Management
Initial Assessment
Follow standard EMS priorities:
- Scene safety
- ABCs
- Level of consciousness
- Airway patency
- Respiratory effort and lung sounds
- Circulation and perfusion
Obtain baseline vital signs including:
- Heart rate
- Respiratory rate
- Blood pressure
- Oxygen saturation
- Blood glucose
- ETCO₂ if available
A “shark fin” waveform on capnography may indicate bronchospasm.
Treatments
Supplemental Oxygen
Oxygen delivery may include:
- Nasal cannula: 2–6 LPM
- Non-rebreather mask: 10–15 LPM
- BVM: 15–25 LPM
Bronchodilators
Albuterol and ipratropium (DuoNeb) help dilate bronchioles and improve airflow. Nebulizer oxygen flow is typically 6–8 LPM.
Corticosteroids
Steroids such as dexamethasone or methylprednisolone help reduce airway inflammation and improve outcomes.
CPAP and BiPAP
Positive pressure ventilation can improve oxygenation, reduce respiratory distress, and decrease the need for intubation. These therapies also help recruit collapsed alveoli.
Epinephrine
Some EMS systems allow epinephrine administration for severe bronchospasm. Providers should follow local protocols and use caution in patients with cardiovascular disease.
Advanced Airway Management
Patients with worsening fatigue, altered mental status, respiratory failure, or arrest may require advanced airway placement. Continue supportive treatments alongside airway management whenever possible.
Transport Considerations
Most hospitals can stabilize COPD exacerbations, but severe cases may require ICU admission and prolonged ventilator support. Oxygen supply and transport distance should always be considered during prolonged transports.
Scenario Summary
A 55-year-old female with COPD develops severe respiratory distress after physical activity in cold weather. She presents with wheezing, accessory muscle use, hypoxia, and tachycardia. EMS administers oxygen, DuoNeb, IV dexamethasone, and cardiac monitoring. The patient improves significantly during transport and is later discharged after hospital evaluation.
This scenario highlights the importance of:
- Early recognition of bronchoconstriction
- Prompt bronchodilator therapy
- Oxygen administration
- Monitoring for respiratory failure
- Preparation for CPAP or advanced airway management if deterioration occurs
Signs of decompensation include:
- Altered mental status
- Fatigue
- Decreased respiratory effort
- Falling oxygen saturation despite treatment
- Inability to speak
- Bradycardia or worsening hypoventilation
and Key Points
- Always prioritize scene safety and ABCs
- Evaluate whether the patient is compensating or decompensating
- Listen carefully to lung sounds
- Recognize accessory muscle use and respiratory fatigue
- Understand respiratory anatomy and gas exchange physiology
- Know all medications within your scope, including indications, contraindications, dosages, and side effects
- Understand the differences between emphysema and chronic bronchitis and how each affects the lungs differently
