Introduction
Hemodialysis is the most common therapy used to manage kidney failure when a kidney transplant is not available. It helps replace essential kidney functions once the kidneys are no longer able to work effectively. These functions include removing waste products, regulating fluid and electrolyte levels, maintaining acid-base balance, and helping control blood pressure.
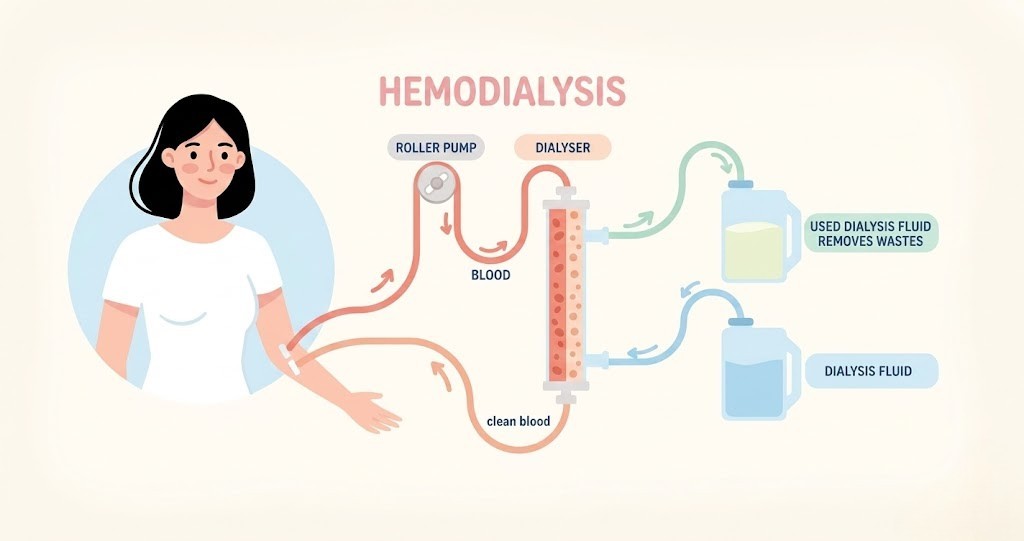
During hemodialysis, the patient is connected to a dialysis machine for several hours multiple times each week. The machine filters the blood to eliminate harmful wastes and excess substances the body can no longer remove independently. Blood is taken from the body through a device called a dialyzer, processed and cleaned in a separate chamber, and then returned to the circulation with waste products removed and electrolyte levels corrected.
Most patients transported for dialysis treatment are not in an emergency condition. However, skipping one or more dialysis sessions can eventually result in severe, potentially fatal complications.
Before routine dialysis can begin, a permanent vascular access site must first be created. Several types of access methods are available depending on the patient’s medical condition and long-term needs.
Dialysis Vascular Access
A dialysis shunt serves as the connection between the hemodialysis access site and a large blood vessel. One common form of access is the arteriovenous (AV) fistula, which is surgically formed by joining an artery directly to a vein. Because dialysis requires repeated access several times weekly, the site must be strong and reliable enough to tolerate frequent use. Creating an AV fistula permanently alters the anatomy of the affected extremity, most often the arm. AV fistulas are generally preferred for long-term dialysis because they carry a lower risk of infection, although they require time to mature before they can be used effectively.
Another option is an AV graft, which connects an artery and vein using synthetic or biological graft material. Unlike fistulas, grafts do not require a maturation period and may be used soon after placement. They are selected based on factors such as the patient’s condition and expected duration of dialysis therapy. Grafts may also serve as temporary access while waiting for a fistula to mature or while awaiting kidney transplantation.
Once vascular access is established, the patient can undergo hemodialysis. During treatment, blood flows through the dialyzer and comes into contact with a cleansing solution called dialysate. Through diffusion and other chemical processes, wastes and excess substances are removed from the blood before it is returned to the body. Dialysate consists mainly of water, salts, and electrolytes.
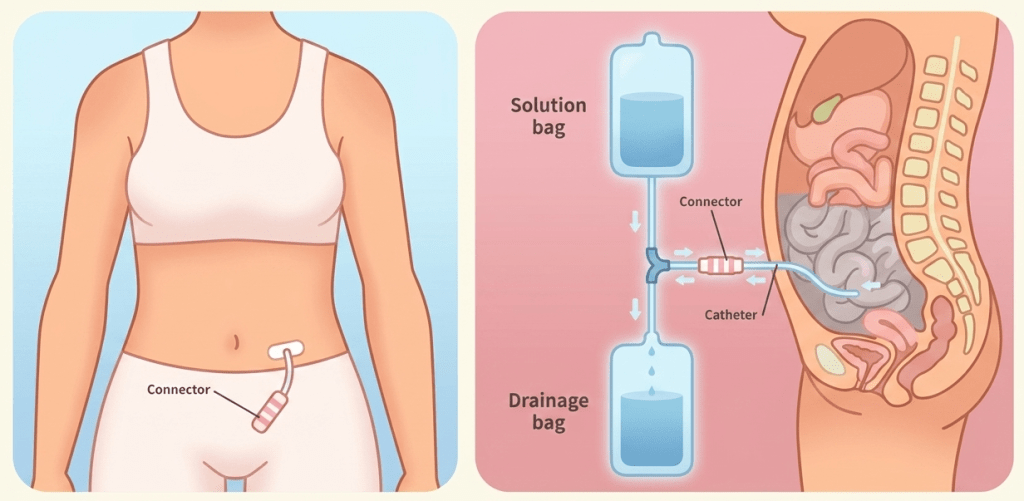
Peritoneal dialysis is another method used to replace kidney function. In this procedure, dialysis solution is introduced into the abdominal cavity, where it remains for several hours to absorb waste products through the peritoneal membrane. The fluid is then drained from the abdomen. A major benefit of peritoneal dialysis is that it can be performed at home rather than in a dialysis center. However, this method carries a greater risk of infection, particularly peritonitis.
Special Considerations
Excessive handling or trauma to an extremity containing a graft or fistula can damage the dialysis access site. Blood pressure measurements, IV insertions, and venipunctures should be avoided in the affected extremity to prevent complications that could require additional surgery for new vascular access. Many dialysis patients also have central venous access devices that provide long-term IV access, reducing the need for peripheral IV placement. Providers should always follow local protocols and consult the patient before using an established access device.
Complications and Adverse Reactions of Dialysis
Although dialysis is a life-sustaining treatment that can significantly prolong survival and, in some cases, support recovery toward kidney transplant, it is not without risks. Some patients tolerate the procedure well, while others may experience complications ranging from mild effects to life-threatening emergencies.
Common Complications and Emergencies
Patients undergoing dialysis may develop a variety of acute or serious complications, including:
- Low blood pressure (hypotension) during or after treatment
- Bleeding (hemorrhage) from an AV fistula or shunt site
- Infections at the vascular access site
- Electrolyte disturbances, especially potassium imbalances
- Air embolism, which can become rapidly life-threatening
- Dialysis machine malfunction, interfering with proper treatment
- Dialysis disequilibrium syndrome, a neurologic reaction that may present with nausea, fatigue, headache, seizures, and altered mental status
In addition to treatment-related issues, long-term dialysis patients are also at higher risk for chronic cardiovascular complications, such as:
- Heart failure
- Myocardial infarction with possible arrhythmias
- Chronic hypertension
- Pericardial effusion leading to tamponade
- Uremic pericarditis
Risks of Missed Dialysis
While dialysis carries risks, failure to attend scheduled treatments can be even more dangerous. Missing even a single session—especially in vulnerable patients—may result in:
- Severe hyperkalemia, often with ECG abnormalities
- Marked muscle weakness
- Fluid overload leading to pulmonary edema
If dialysis is not continued at all, the patient may progress into end-stage renal failure complications, which can be fatal.
Management of Dialysis-Related Emergencies
The priority in any acute dialysis emergency is stabilization using the ABCs (airway, breathing, circulation). These foundational steps should always be reassessed first, especially if the patient is critically ill.
- Hypotension: Administer fluids as indicated and monitor hemodynamic status closely.
- Bleeding from access site: Apply firm direct pressure; a vascular clamp may be used if available in dialysis settings.
- Electrolyte imbalance: Treat based on ECG findings and established protocols. For example, bradycardia from low potassium may require atropine, while symptomatic high potassium may be treated with calcium or sodium bicarbonate per orders.
- Pulmonary edema: Provide oxygen and consider positive pressure ventilation if needed; elevate the head of the bed.
- Signs of poor perfusion: Position the patient flat to improve circulation when appropriate.
Ultimately, most dialysis emergencies require rapid supportive intervention and prompt transport to a higher level of care for continued management of both acute and chronic complications.
