Anatomy and Physiology Review
The nervous system is divided into two main parts: the central nervous system (CNS) and the peripheral nervous system (PNS). The brain and spinal cord make up the CNS. Within the brain, there are two primary cell types: neurons and glial cells. Neurons are responsible for transmitting electrical and chemical signals throughout neural pathways, while glial cells provide structural support, nourishment, and protection for neurons.
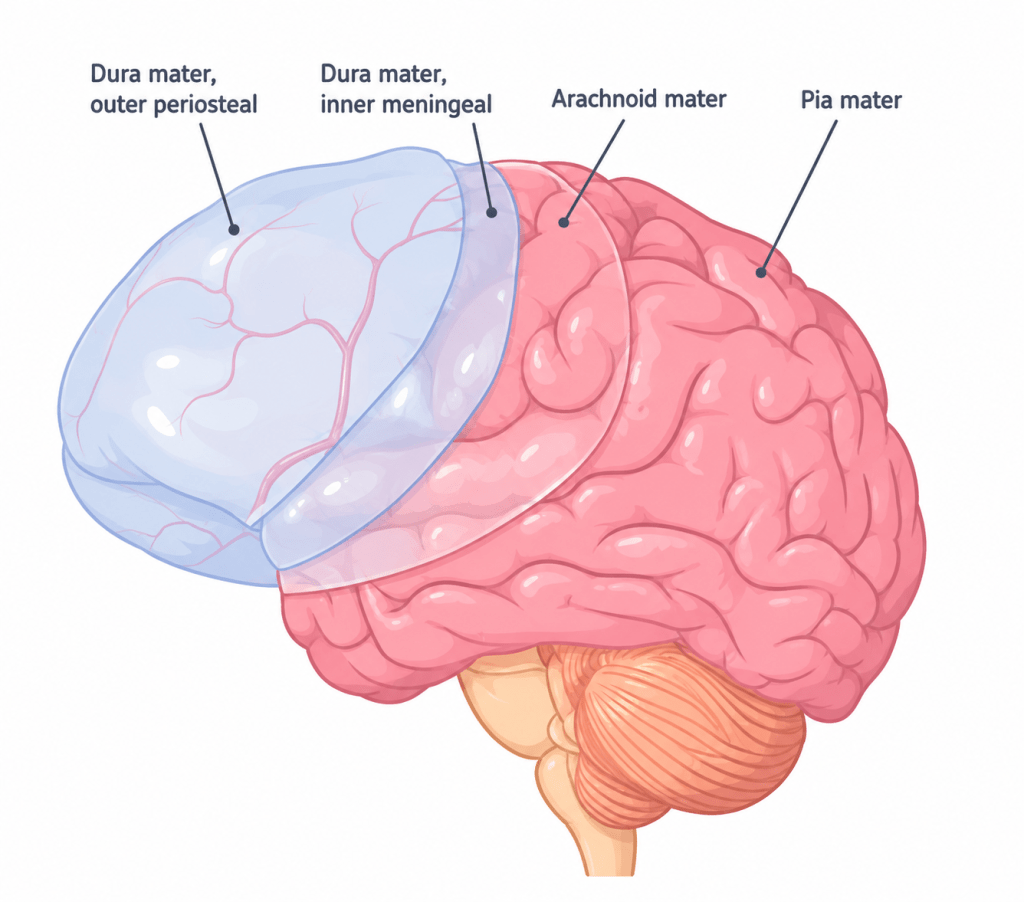
The skull protects the brain and is composed of the cranium and facial bones. Between the skull and brain are three protective layers known as meninges. From outermost to innermost, these are the dura mater, arachnoid mater, and pia mater. The space between the dura and arachnoid mater is the subdural space, while the space between the arachnoid and pia mater is the subarachnoid space.
The spinal cord extends upward into the brainstem, which is made up of the midbrain, pons, and medulla oblongata. The brainstem is responsible for transmitting signals between the brain and body and plays a critical role in regulating breathing, blood pressure, and consciousness.
Located at the back of the brain is the cerebellum, which is responsible for coordination and fine motor control. Above it lies the occipital lobe, which processes visual information. The parietal lobes integrate sensory input and help with spatial awareness and memory formation. Adjacent to them are the temporal lobes, which are involved in language comprehension, facial recognition, and object identification.
Recognition
While brain anatomy is extensive, EMS providers focus on recognizing problems rather than mastering all details. Brain dysfunction is most commonly seen as altered mental status (AMS). In some cases, the cause is obvious, such as head trauma, while in others, it requires systematic evaluation.
A common tool used in prehospital care is the mnemonic AEIOU-TIPS:
- A: Alcohol, acidosis
- E: Environmental exposure, epilepsy, electrolytes imbalance, encephalopathy, endocrine disorders
- I: Infection
- O: Oxygen deficiency, overdose
- U: Uremia, underdose
- T: Trauma
- I: Insulin-related issues, intestinal causes
- P: Poisoning, psychogenic causes
- S: Stroke, shock
Another useful assessment tool is “Oxygen, Glucose, Pump, SITS”:
- Oxygen: Check oxygen saturation
- Glucose: Check blood sugar levels
- Pump: Assess heart rate, rhythm, and ECG
- S: Structural causes such as stroke or trauma
- I: Infection such as sepsis
- T: Toxins such as drug overdose
- S: Social or psychiatric causes after medical causes are ruled out
Using structured approaches helps narrow down the cause of AMS efficiently.
Treatment
Management of AMS begins with identifying and treating the underlying cause. Depending on the situation, interventions may range from oxygen therapy and IV glucose administration to advanced airway management and rapid sequence intubation.
Scenario
You respond to a call at a public park where a man in his mid-twenties is found unconscious on the ground. Two empty beer cans are nearby. The scene is safe.
After ensuring BSI and scene safety, you perform a primary assessment. The patient has an open airway but irregular respirations and a slow, strong radial pulse. He responds only to painful stimuli.
Using the AEIOU-TIPS approach:
- A (Alcohol/acidosis): Alcohol use is present, but the amount seems insufficient to explain his condition. No signs of acidosis.
- E (Environmental/epilepsy/electrolytes/etc.): Patient is warm, no seizure signs, and no obvious metabolic or endocrine issues.
- I (Infection): No infection source identified.
- O (Oxygen/overdose): Oxygen saturation is 99% on room air. No evidence of overdose or drug paraphernalia.
- U (Uremia/underdose): No medication bottles or renal disease signs present.
- T (Trauma): On full exam, a depressed skull fracture is identified at the posterior head. This is the likely cause.
- I (Insulin/intestinal): Blood glucose is normal.
- P (Poison/psychogenic): No toxins or psychiatric indicators noted.
- S (Stroke/shock): Stroke scale is inconclusive, but traumatic brain injury is evident.
The patient is determined to have a severe head injury and should be transported immediately to a trauma center. Establish IV access, secure the airway with intubation if needed, and manage ventilation carefully. Mild hyperventilation may be used to help reduce intracranial pressure by lowering CO₂ levels.
Transport should be rapid and prioritized (code 3), as definitive care will require neurosurgical intervention.
Final Thoughts
Family members and bystanders are valuable sources of information in AMS cases. They may provide details about when symptoms started, prior episodes, or relevant events leading up to the change in mental status. This information is critical, especially once the patient is transported and no other reliable historian is available.
