Introduction
Breathing is the process of moving air into and out of the lungs to exchange gases between the body and the environment. During inhalation, oxygen enters the lungs and diffuses into the bloodstream. During exhalation, carbon dioxide moves from the bloodstream into the lungs so it can be released into the atmosphere.
This topic reviews the anatomy and physiology involved in breathing and explains how disruptions in ventilation or gas exchange can quickly become life-threatening.
Ventilation vs. Respiration
Ventilation
Ventilation refers to the physical movement of air into and out of the lungs.
Respiration
Respiration refers to the exchange of oxygen and carbon dioxide at the cellular level between the lungs and bloodstream.
Ventilation
Muscle Involvement
Inhalation
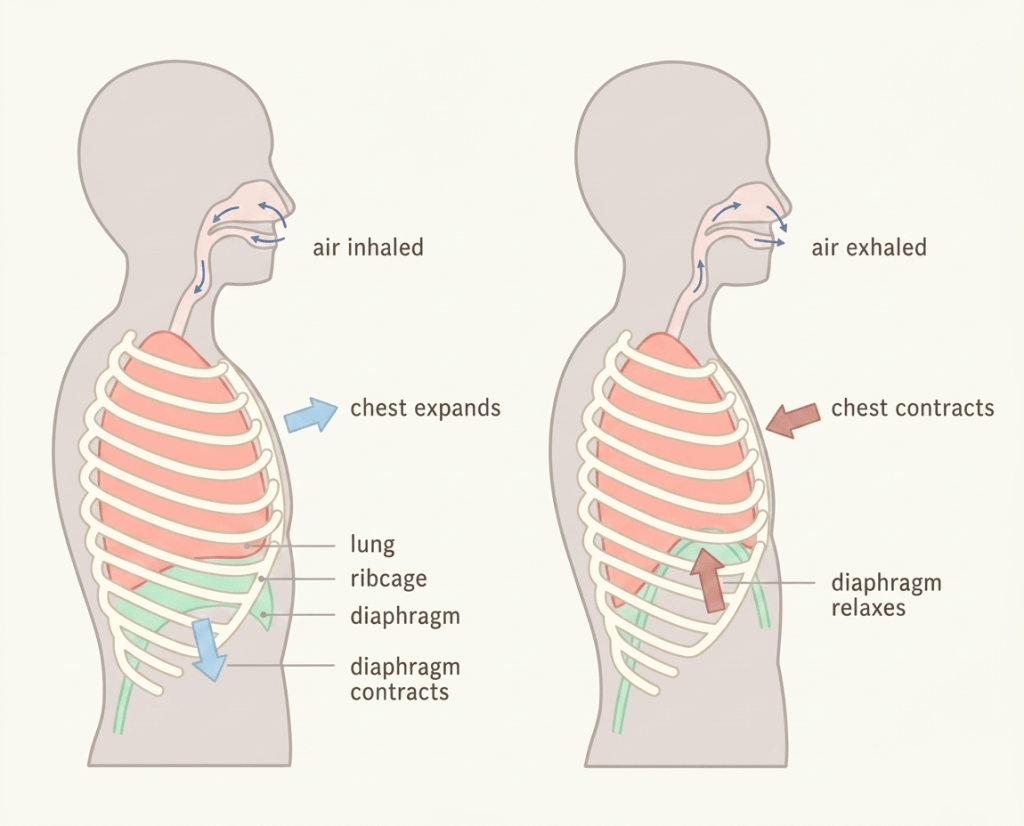
During inhalation:
- The diaphragm contracts and flattens downward.
- The intercostal muscles contract, lifting the rib cage upward and outward.
- The thoracic cavity expands in size.
- As chest volume increases, intrathoracic pressure decreases.
- When intrathoracic pressure becomes lower than atmospheric pressure, air is drawn into the lungs.
Exhalation
During exhalation:
- The diaphragm and intercostal muscles relax.
- The chest cavity returns to its resting size.
- As thoracic volume decreases, intrathoracic pressure rises.
- Air is forced out of the lungs to equalize pressure with the atmosphere.
Respiration
During respiration:
- Oxygen diffuses from the alveoli into the pulmonary capillaries.
- Carbon dioxide diffuses from the bloodstream into the alveoli to be exhaled.
- This exchange occurs across the alveolocapillary membrane, which is a thin, single-cell layer separating the lungs from the bloodstream.
Anatomy of the Upper and Lower Airway
Upper Airway Anatomy
Nasal Cavity
The uppermost portion of the airway responsible for filtering, warming, and humidifying inhaled air.
Oral Cavity
Includes the cheeks, tongue, hard palate, and soft palate, allowing airflow through the mouth.
Pharynx
A muscular passageway extending from the back of the nasal and oral cavities to the esophagus and larynx.
Larynx
A complex airway structure connecting the pharynx to the trachea and containing the vocal cords.
Lower Airway Anatomy
Trachea
- The first structure of the lower airway.
- Approximately 10–12 cm long.
- Connects the larynx to the right and left mainstem bronchi.
- Supported by C-shaped cartilage rings that help maintain airway patency.
Bronchi and Bronchioles
- The bronchi divide into smaller bronchioles that direct airflow deeper into the lungs.
Alveoli
- Tiny air sacs located at the ends of the bronchioles.
- Primary site of gas exchange.
Pleural Membranes
- Thin membranes surrounding the lungs.
- Help attach the lungs to the chest wall and allow smooth lung movement during breathing.

Recognizing Respiratory Complications
Problems with Respiratory Rate
Tachypnea
A respiratory rate greater than 20 breaths per minute is considered abnormally fast and may indicate respiratory distress or metabolic compensation.
In some situations:
- The respiratory problem itself must be treated.
- In others, the body is compensating for another condition such as metabolic acidosis.
Bradypnea
A respiratory rate less than 12 breaths per minute is considered abnormally slow and may indicate respiratory depression or impending respiratory failure.
Apnea
Absence of breathing requires immediate intervention with positive pressure ventilation (PPV).
Inadequate Ventilation
Ventilation may also be inadequate if:
- Breaths are too shallow.
- Respiratory rate is too slow or too fast.
- Tidal volume is insufficient.
These situations may require assisted ventilations using a bag-valve mask (BVM).
Other Signs and Symptoms of Respiratory Complications
Labored Breathing
Increased effort during respirations may indicate respiratory distress.
Diaphragmatic Breathing
Use of abdominal muscles during breathing may suggest respiratory fatigue or distress.
Adventitious Lung Sounds
Crackles
Often indicate fluid within the alveoli and may occur with:
- Congestive heart failure (CHF)
- Pneumonia
Stridor
A high-pitched upper airway sound indicating airway obstruction.
Wheezing
Usually caused by lower airway constriction such as:
- Asthma
- COPD
- Allergic reactions
Rhonchi
Low-pitched gurgling or snoring sounds associated with mucus in the larger airways.
Bronchospasm
Bronchospasm occurs when smooth muscles surrounding the bronchioles constrict, narrowing the airway.
Common causes include:
- Asthma
- COPD
- Allergic reactions
Pulmonary Edema
Pulmonary edema is fluid accumulation within the lungs that interferes with gas exchange.
Common causes include:
- Congestive heart failure (CHF)
- Pneumonia and lower respiratory infections
Scenario
Dispatch Information
You are dispatched code 3 to a residence for a 20-year-old female experiencing respiratory distress. Dispatch reports the scene is secure.
Scene Information
Upon arrival, standard BSI precautions are taken. The patient is found seated upright in Fowler’s position on the couch.
Patient Assessment
The patient appears tachypneic with labored breathing. She reports a severe history of asthma and states she used her albuterol inhaler twice earlier in the morning without relief.
Auscultation reveals bilateral expiratory wheezing.
Vital signs:
- Respiratory rate: 24 breaths/minute
- Other vital signs: within normal limits
Treatment
Initial treatment includes:
- Supplemental oxygen
- Request for ALS intercept if symptoms fail to improve
ALS interventions may include:
- Nebulized bronchodilators
- IV corticosteroids
- Advanced airway management if respiratory failure develops
Expected Reassessment Findings
Following treatment, expected improvements may include:
- Reduced work of breathing
- Lower respiratory rate
- Improved SpO₂ levels
- Decreased wheezing
- Relaxation of airway smooth muscle
- Mild increase in heart rate secondary to albuterol administration
