Introduction
A stroke is a medical condition caused by a sudden interruption of blood flow to the brain. There are two primary types of stroke: ischemic and hemorrhagic. Stroke is one of the leading causes of death in the United States and is the primary cause of long-term disability.
Ischemic Stroke
Ischemic strokes occur when blood flow to the brain is blocked by a clot, preventing oxygen and nutrients from reaching brain tissue. Without adequate blood supply, brain cells begin to die.
Ischemic strokes are further divided into:
- Thrombotic strokes, which occur when a clot forms within a blood vessel in the brain
- Embolic strokes, which occur when a clot forms elsewhere in the body and travels to the brain, becoming lodged in a vessel
Ischemic strokes account for approximately 87% of all stroke cases.
Hemorrhagic Stroke
Hemorrhagic strokes occur when a blood vessel in or around the brain ruptures, leading to bleeding within brain tissue or surrounding spaces. This bleeding reduces oxygen delivery and damages brain cells.
In addition, hemorrhage can increase intracranial pressure (ICP), which may result in brain swelling and further neurological injury due to reduced blood flow and oxygenation. Hemorrhagic strokes make up roughly 13% of all strokes.
Stroke Recognition Tools
Stroke is commonly associated with sudden neurological changes and altered mental status. Key warning signs include:
- Sudden confusion or disorientation
- Changes in mental status
- Loss of coordination or balance
- Visual disturbances
- Weakness or numbness of the face, arm, or leg, typically on one side
- Sudden severe headache, sometimes described as “worst headache”
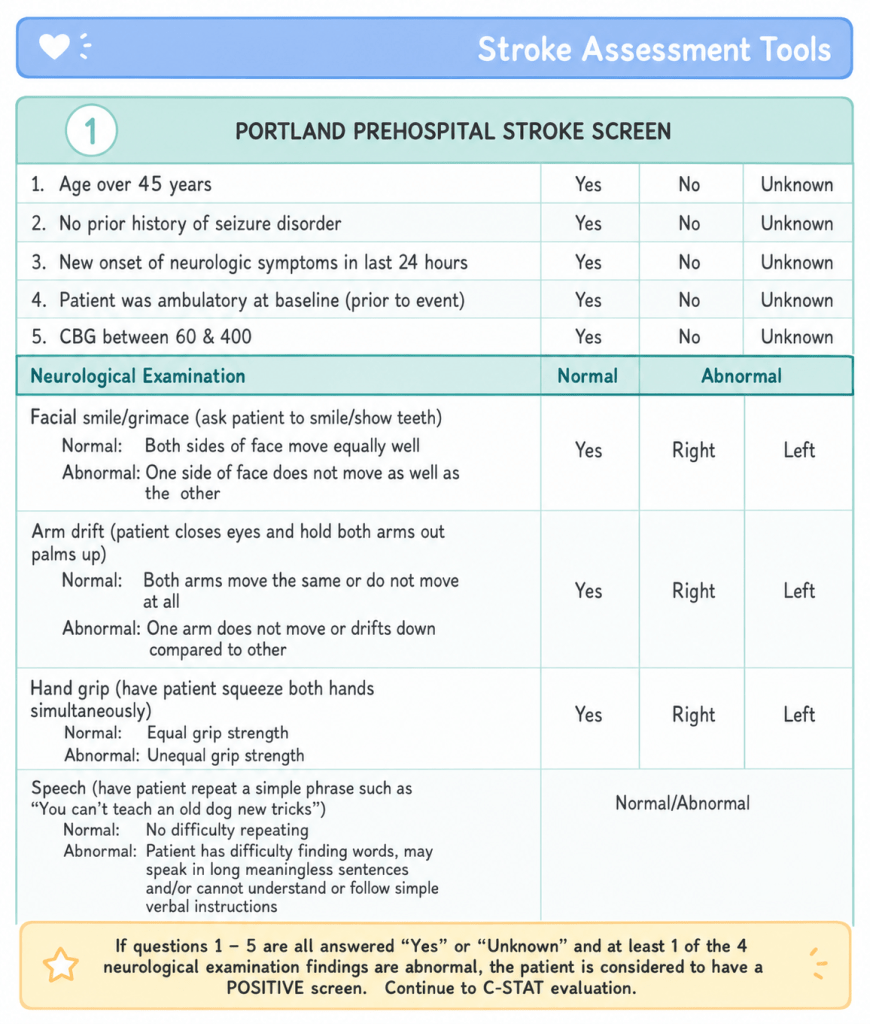
Prehospital providers use structured screening tools to help identify stroke, such as the Cincinnati Prehospital Stroke Scale (CPSS). This tool evaluates facial droop, arm drift, and speech abnormalities. Many EMS systems expand on this with additional protocols, such as the Portland Prehospital Stroke Screen, which first rules out other causes of altered mental status before activating a stroke alert.
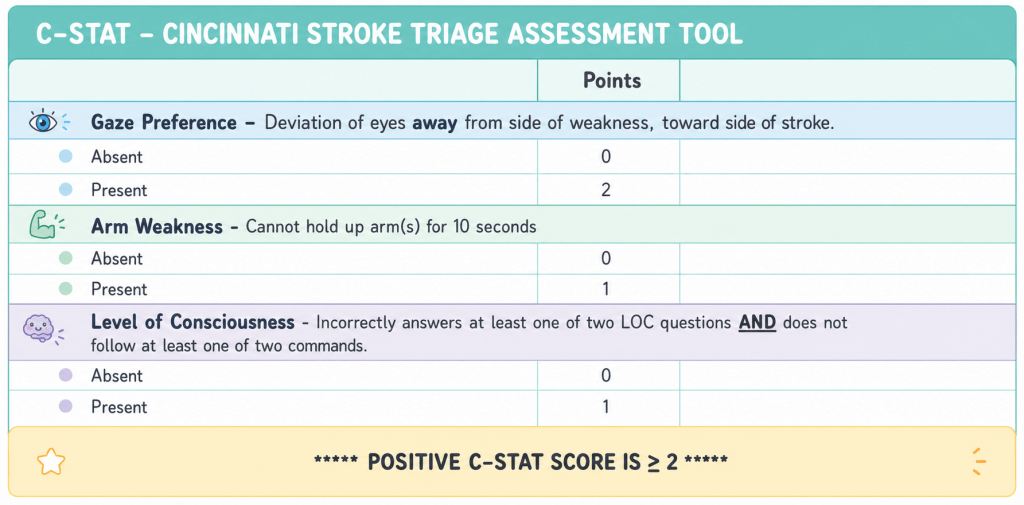
If a stroke is suspected, further assessment may include tools like the Cincinnati Stroke Triage Assessment Tool (CSTAT), which helps identify possible large vessel occlusion. A positive CSTAT result suggests the need for transport to a facility capable of advanced stroke interventions, such as mechanical thrombectomy.
Prehospital Management
Initial management begins with scene safety and a rapid primary assessment, with immediate attention to airway, breathing, and circulation. Because stroke is time-sensitive, evaluation should not be delayed.
Key steps include:
- Rapid assessment of altered mental status
- Performing CPSS or similar stroke screening tool
- Checking blood glucose to rule out hypoglycemia
- Monitoring blood pressure, oxygen saturation, and cardiac rhythm
- Considering alternative causes such as infection, trauma, or toxic exposure
Once stroke is suspected, definitive treatment cannot be provided in the field. The priority becomes rapid transport to an appropriate hospital. Minimizing on-scene time is critical to preserve brain tissue.
Choosing the correct facility is essential, as some hospitals are equipped for advanced stroke interventions, while others are not. Local protocols should guide destination decisions.
If ALS is available, establishing a large-bore IV (typically 18 gauge or larger) may assist with hospital diagnostics and imaging procedures.
Example Scenario Summary
A 55-year-old male presents with sudden slurred speech and left-sided facial droop. Vital signs are stable, oxygen saturation is normal, and blood glucose is within normal range. No signs of infection, trauma, or drug use are identified. Stroke screening is positive on CPSS, and CSTAT indicates inability to follow commands and hold arms up, suggesting a possible large vessel occlusion.
Rapid transport is initiated to the nearest appropriate stroke center. The patient is continuously monitored, IV access is established if possible, and neurological status is reassessed en route.
Final Thoughts
Emergency medical providers cannot definitively treat stroke in the field. Their most important role is early recognition, rapid assessment, and minimizing delays to hospital care. Early identification and fast transport significantly improve outcomes by reducing the time brain tissue is deprived of oxygen.
